
Our May focus is an article in JVDI’s May issue, in the Special Section on equine gastrointestinal diseases in horses: “Gastrointestinal biopsy in the horse: overview of collection, interpretation, and applications” by Jesse M. Hostetter, Francisco A. Uzal.
J Vet Diagn Invest 2022;34(3). https://journals.sagepub.com/doi/full/10.1177/10406387221085584
Abstract. Evaluation of gastrointestinal (GI) biopsies is a multistep process that includes reviewing an appropriate history, determining sample quality, and evaluating histologic sections. Selected diagnostic parameters that, in combination with intestinal histopathology, can be useful to localize disease to the intestinal tract in the horse include hypoproteinemia and hypoalbuminemia, ultrasound evidence of increased thickness of the small intestinal wall, and alterations in glucose or D-xylose absorption tests. Biopsies may be acquired either endoscopically, or via laparoscopy or standing flank incisional approaches. GI sections should be evaluated using a systematic approach that includes both architectural changes and inflammatory cell infiltrates. Although strategies have been developed for assessment of GI biopsies from the dog and cat, a standardized approach to interpretation of the equine GI biopsy has yet to be developed. GI biopsies pose several challenges to the pathologist, especially for endoscopic biopsies in which the quality of the specimen and its orientation may vary greatly. Architectural changes are arguably the most critical changes to evaluate. In a horse with chronic GI inflammation, such as occurs in idiopathic inflammatory bowel disease (IBD), the cell types encountered frequently are macrophages, eosinophils, lymphocytes, and plasma cells. Increased numbers of these cell types are categorized loosely as mild, moderate, and severe. Specific forms of idiopathic IBD have been further classified by this infiltrate as granulomatous enteritis, eosinophilic enteritis, and lymphoplasmacytic enteritis; there is limited information on microscopic changes with each. Unfortunately, microscopic GI lesions are usually nonspecific, and determination of etiology requires further investigation.
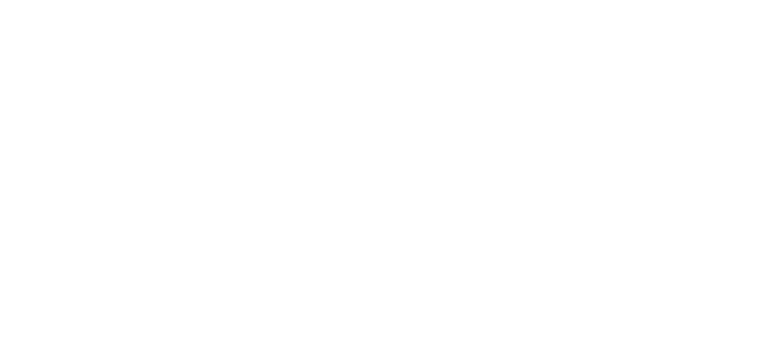
Figures 1–6. Equine gastrointestinal biopsies. Figure 1. Gastric endoscopic biopsy showing only mucosa sectioned tangentially. H&E. Figure 2. Colon surgical biopsy, including full thickness of the colonic wall. H&E. Figure 3. Duodenal surgical biopsy. This biopsy is mostly free of artifact and well oriented, so that numerous villus-crypt units with associated lamina propria can be evaluated. H&E. Figure 4. Gastric endoscopic biopsy that includes only the superficial aspect of the mucosa with artifactually detached mucosal epithelium. H&E. Figure 5. Duodenal endoscopic biopsy with severe crushing artifact. H&E. Figure 6. Duodenal biopsy with muscularis and serosa, but missing mucosa and submucosa. H&E.
JVDI News
Be sure to sign up for JVDI email alerts! JVDI alerts let you know when new articles and eTOCs are available online. Alerts can be requested on a daily, weekly, or monthly basis. Note that only abstracts are available via email alerts—you will need to login through AAVLD or your institution to access and read the full articles.
Signing up for email alerts is simple.
1. Go to the JVDI website: https://journals.sagepub.com/home/vdi
2. On the Stay Connected tab dropdown menu, click on Email Alerts
3. Choose New Content and/or Announcements, then Create Email Alert
4. Then “Sign in to SAGE Journals”
If you already have a SAGE account, use the left box My Account. Otherwise, click Register for a free SAGE Journals account. (You will be able to update your email alerts anytime and will see the message “Your email alert settings have been updated” at completion.)
Let’s stay connected!


